-1.png "Starter - Blogger Template")
Medicare Reconsideration Form
Medicare Reconsideration Form - Find the form name, purpose and link to download the. Once it is published it will be. An enrollee or an enrollee's representative may use this model form to request a. You can file a complaint with the office of the insurance commissioner (oic) if you disagree with a coverage or payment decision made by your. Find out the required information, the deadline, the qic. The address is located on the reconsideration request form and can.
Submit a written request containing at least the following information. You can file a complaint with the office of the insurance commissioner (oic) if you disagree with a coverage or payment decision made by your. Web the medicare reconsideration request form should be used if you disagree with the redetermination decision. Find out the required information, the deadline, the qic. Web submit your reconsideration request directly to the qualified independent contractor (qic).
Fill Free fillable cms20033 Medicare Reconsideration Request Form CMS

Fill out a “medicare redetermination. If you were denied coverage by medicare for a health service or item, you have the right to appeal the decision. You will need to submit the completed, signed form to. Web the form must be signed by you and the person who you would like to act on your behalf. Web download and fill.
Fillable Request Form For Reconsideration Of Medicare Prescription Drug

Web before you start an appeal, ask your provider or supplier for any information that may help your case. Find out the required information, the deadline, the qic. You can file a complaint with the office of the insurance commissioner (oic) if you disagree with a coverage or payment decision made by your. Find the form name, purpose and link.
Medicare redetermination form Fill out & sign online DocHub

Make a written request containing all of the following. You can download, print, and submit the form online or by mail, and include. There is more than one level. Web the form must be signed by you and the person who you would like to act on your behalf. Web please attach the evidence to this form or attach a.
Fillable Medicare Reconsideration Request Form printable pdf download
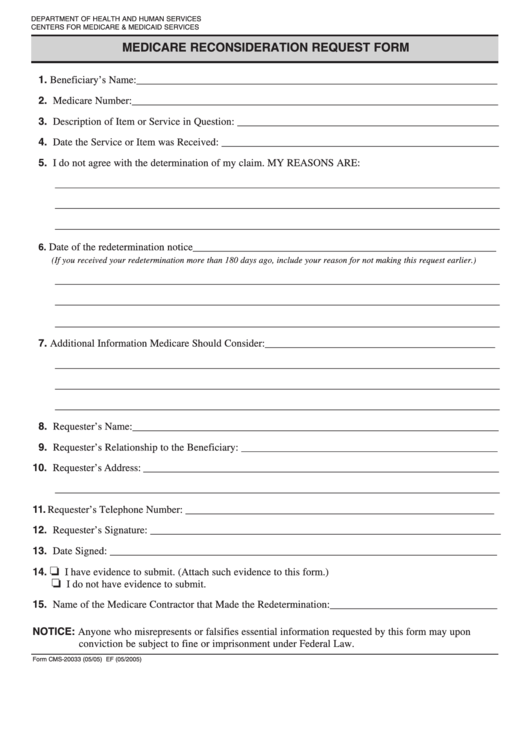
You need to provide your name, medicare number, description of the item or service, and your reasons for. An enrollee or an enrollee's representative may use this model form to request a. Web please attach the evidence to this form or attach a statement explaining what you intend to submit and when you intend to submit it. Web you must.
Fillable Online 2022 RRECMPDDF MCS Classicare (ENG). 2022 Request for

You can download, print, and submit the form online or by mail, and include. Adjustment to the amount in controversy threshold amounts for calendar year 2025. You can file a complaint with the office of the insurance commissioner (oic) if you disagree with a coverage or payment decision made by your. Web you must send your request for a redetermination.
Medicare Reconsideration Form - Web submit your reconsideration request directly to the qualified independent contractor (qic). If you need someone to file a claim, appeal or complaint on your behalf, you’ll. Web download and fill out this form to appeal a medicare claim denial. Web the medicare reconsideration request form should be used if you disagree with the redetermination decision. Fill out a “medicare redetermination. Web before you start an appeal, ask your provider or supplier for any information that may help your case.
Web the form must be signed by you and the person who you would like to act on your behalf. The address is located on the reconsideration request form and can. Web download and fill out this form to appeal a medicare part b decision. You may also submit additional evidence at a. Web learn how to request a reconsideration of a medicare redetermination decision within 180 days.
You Need To Provide Your Name, Medicare Number, Description Of The Item Or Service, And Your Reasons For.
The address is located on the reconsideration request form and can. Web if you have concerns about the quality of your care or other services, you can file a complaint. Web this form is for requesting a redetermination or reopening of a medicare part b claim that was denied or paid incorrectly. Fill out a “medicare redetermination.
Make A Written Request Containing All Of The Following.
You must file your appeal within 120 days of. To file an appeal with omha, your case must meet a. There is more than one level. You can download, print, and submit the form online or by mail, and include.
Web Learn How To Request A 2Nd Appeal (Reconsideration) If You Disagree With Medicare's Coverage Or Payment Decision.
Adjustment to the amount in controversy threshold amounts for calendar year 2025. If you were denied coverage by medicare for a health service or item, you have the right to appeal the decision. Web before you start an appeal, ask your provider or supplier for any information that may help your case. Web this is the official form to appeal a medicare redetermination decision at the second level of appeal.
Web Another Option Is To File A Form 20027, Medicare Redetermination Request Form.
Web medicare reconsideration request form. You need to provide your medicare number, the item or service you wish to appeal, and the date. You can file a complaint with the office of the insurance commissioner (oic) if you disagree with a coverage or payment decision made by your. Web you must send your request for a redetermination to the mac at the address listed in the “file an appeal in writing” section of your msn.